MSK system
Protocols
Normal Level :
- Male = 4.0 to 8.5 mg/dL
- Female = 2.7 to 7.3 mg/dL
- Old people = Values may be slightly increased.
- Child = 2.5 to 5.5 mg/dL
- Newborn = 2.0 to 6.2 mg/dL
Increased Uric Acid Level
(Hyperuricemia >7 Mg/DL In Males And >6 Mg/DL In Female) Is Seen In:
- Gout.
- renal diseases and Renal failure, prerenal Azotemia.
- Alcoholism.
- Lead poisoning.
- Leukemia, Multiple Myeloma, Lymphoma.
- Starvation, weight-loss diets.
- Metabolic acidosis. and Diabetic ketoacidosis
- Toxemia of pregnancy.
- Liver diseases.
- Hemolytic Anaemia.
- Following excessive cell destruction, as in chemotherapy and radiation therapy.
- Lead poisoning.
- Alcoholism.
- Hereditary gout.
- Hyperlipidemia and obesity.
- Hypothyroidism.
- Hypoparathyroidism.
- Hemolytic anemias.
- Psoriasis.
- Glycogen storage disease.
- Increased ingestion of purines in diet e.g. liver, sweetbreads, kidneys, and anchovies.
- A genetic inborn error in purine metabolism.
- Metastatic cancers.
- Rhabdomyolysis e.g. Heavy Exercise, Crush injury, burns, epileptic seizure, and myocardial infarction.
Hyperuricemia Due To Decreased Excretion:
- Primary:
- Idiopathic.
- Secondary:
- Acidosis in diabetes and starvation.
- Hypothyroidism.
- Toxemia of pregnancy.
- Shock or chronic blood loss.
- Alcoholism.
- Hyperlipoproteinemia.
- Acute and Chronic renal failure.
- Lead poisoning.
- Salicylate due to low doses.
- Thiazide diuretics.
Decreased Level Of Uric Acid Seen In (Hypouricemia <2 Mg/DL) :
- Fanconi’s syndrome
- Wilson’s disease
- Some malignancies like Hodgkin’s lymphoma and Myeloma.
- Deficiency of xanthine oxidase.
- Lead poisoning.
- Yellow atrophy of the liver.
- Salicylates in low doses.
- Thiazide diuretics.
- Increased renal reabsorption.
Diseases with positive antinuclear antibodies:
| Diseases | Positivity of ANA % | another source of positivity % | Another source of positivity % |
|---|---|---|---|
| SLE | 95 | 90 to 100 | >95 |
| Drug-induced lupus erythematosus | >95 | ||
| Sjogren’s syndrome | 60 | 85 | 75 to 90 |
| Scleroderma | 70 | 88 | 70 to 90 |
| Dermatomyositis | 30 | 40 to 60 | |
| Rheumatoid arthritis | 30 | 55 | Rare |
| Polyarteritis | 10 | ||
| Juvenile arthritis | 22 | ||
| Mixed connective tissue disease | 100 | >95 | |
| CREST syndrome | 70 to 90 |
The Positive Or Increased Level Of ANA Is Seen In:
- SLE.
- Rheumatoid arthritis.
- Polyarteritis Nodosa
- Dermatomyositis.
- Sjogren’s syndrome.
- Other autoimmune diseases.
- Cirrhosis.
- Chronic hepatitis.
- Leukemia.
- Scleroderma.
- Multiple sclerosis.
- Infections.
- Malignancies.
Normal Aldolase level
- Adult = 1.0 to 7.5 U /L
- Newborn = 4 x adult level
- Values are double in early childhood and then slowly fall to a normal level by the 18 to 20 years of age.
- Children 10 to 24 months = 3.4 to 11.8 U/L
- child 25 months to 16 years = 1.2 to 8.8 U/L
The Aldolase level is increased in:
- Cell destruction like Acute myocardial infarction (5 to 8 times the normal).
- Burns.
- Acute Hepatitis (Viral or toxic). It is raised in the early stage of viral or toxic hepatitis.
- Inflammatory diseases of muscles (Myopathy).
- Raised in skeletal muscle disease or injury.
- Raised in Muscular dystrophy. It is raised in pseudo hypertrophic muscular dystrophy (as the CPK is also raised).
- Duchenne’s muscular dystrophy.
- Trauma involving the muscles.
- Carcinoma of the prostate (about 6 times the normal).
- Cancer involving the lung, breast, liver, GIT, or genitourinary system.
- Myelocytic leukemia (about 6 times the normal).
- Megaloblastic and hemolytic anemia (about 10 to 13 times the normal).
- In neoplastic diseases like carcinomatous metastasis to liver, lung, breast, genitourinary system, melanoma, and CNS tumors.
- This may be raised in eosinophilia-myalgia syndrome.
- Trichinosis.
- Hemolytic anemia.
- Gangrene.
- Melanoma.
Normal Aldolase level:
- Neurogenic muscle atrophy.
- Cirrhosis (or maybe slightly increased).
- Obstructive jaundice (or maybe slightly increased).
Decreased Aldolase level is seen in:
- Hereditary fructose intolerance.
- This may indicate late muscular dystrophy.
- This test is nonspecific, so not commonly requested except for follow-up on muscle diseases.
- This is also not recommended due to the CPK raised level in all these conditions where aldolase is raised.
Normal Anti-DsDNA Antibodies:
- Negative : < 70 IU/mL
- Borderline : 70-200 IU/mL
- Positive : > 200 IU /mL
Increased Anti-DNA antibody level seen in:
- Systemic lupus erythematosus.
- Other autoimmune diseases.
- Biliary Cirrhosis.
- Chronic hepatitis.
- Infectious mononucleosis.
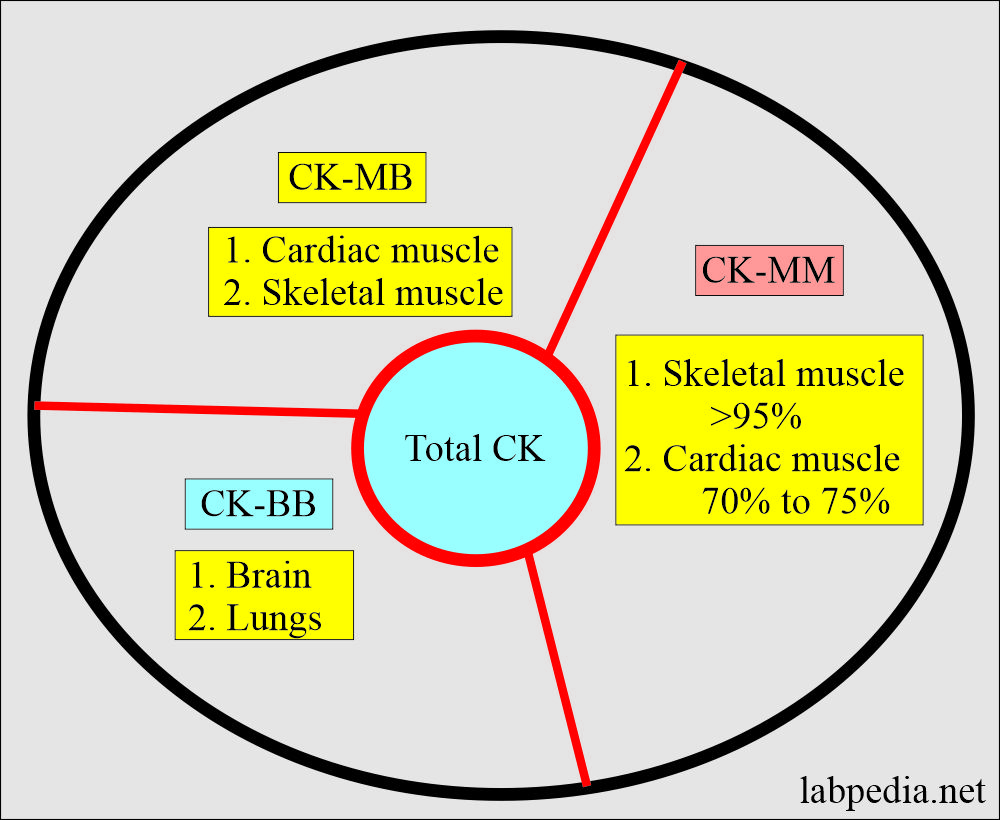
Raised level of CK-MB:
- Acute myocardial infarction.
- Cardiac surgery (e.g., an aneurysm ).
- cardiac defibrillation.
- Myocarditis.
- cardiac ischemia.
- ventricular arrhythmias
Raised level of CK-MM:
- Muscular dystrophy.
- Rhabdomyolysis.
- Myositis.
- Recent injury.
- Intramuscular injection.
- Trauma and crushing injuries.
- Hypothyroidism.
- Shock.
Raised level of CK-BB:
- Brain Injury.
- Brain cancers.
- Cerebrovascular accidents.
- Subarachnoid hemorrhage.
- Shock.
- Seizure.
- Adenocarcinoma, especially lung and breast.
- Pulmonary infarction.
- Normal values are found in myasthenia gravis and multiple sclerosis.
Pathophysiology of Human Leucocyte Antigen B27
- The major histocompatibility antigen in humans belongs to the presence of these antigens on the surface of white cells and the so-called HLA (human leukocyte antigen).
- These are present in the nucleated cells and platelets and are mostly detected in lymphocytes.
- HLA-Ag is present in minimal concentration to the absent expression on the RBCs.
- These antigens are labeled at HLA- A, B, C, and D.
- The presence or absence of these genes is present on chromosome 6.
- HLA-B27 is found in 90 % of patients with ankylosing spondylitis.
- HLA-B27 is also present in the normal population in 5% to 7 %.
- HLA-B27 is also found in other diseases like Reiter’s syndrome, Anterior uveitis, and Grave disease.
Normal Of Human Leucocyte Antigen B27
- HLA-B27 is negative.
Positive Human Leucocyte Antigen B27 Seen In:
- Ankylosing spondylitis.
- In close relatives of the patients, it is found in increased frequency.
- Reiter syndrome.
- Grave’s disease.
- Anterior uveitis.
- Chronic active hepatitis.
- Multiple sclerosis.
- Myasthenia gravis.
- Psoriasis.
- Rheumatoid arthritis.
- Celiac disease.
- Juvenile diabetes.
- Hemochromatosis.
Diagnosis:
- Rheumatoid factor is used to diagnose Rheumatoid Arthritis.
- This factor consists of a group of immunoglobulin reacting with the Fc region of IgG. This may be IgM, or IgG, or IgA.
- RA factor is present in:
- Blood
- Joint fluid
- It first appears in the joint fluid then in the blood.
Limitations
- 70-90% of the cases are positive for rheumatoid arthritis.
- A negative result does not rule out rheumatoid arthritis.
- The false-positive test may be seen in:
- 71% Rheumatic fever.
- 30-40% SLE.
- 12% Gout
- RA factor may be positive in tuberculosis & syphilis.
- False Positive may also be seen in old age, liver disease, SBE, chronic lung disease & syphilis.
Introduction :
- The technique of dual energy X-ray absorptiometry (DEXA) works on the principle that calcium in bone attenuates passage of X-ray beams through the tissue. It is usually performed at the lumbar spine and hip, and provides images of the region studied.

Indications :
- 1. Diagnosis and management of osteoporosis.
- 2. Radiographic osteopenia
- 3. Previous fragility fracture (in those aged <75 years)
- 4. Glucocorticoid therapy (in those aged <65 years)
- 5. Body mass index <19 (kg/m2)
- 6. Maternal history of hip fracture
- 7. BMD-dependent risk factors in
Normal value :
- Most DEXA scanners give result expressed as grams of hydroxyapatite/cm2, and as a T-score and Z-score value.
Interpretation :
- The BMD T-score is the standard deviations by which the value differs from the value of a young healthy control.
- The BMD Z-score is the standard deviations by which the value deviates from the value of agematched controls.
- Osteoporosis: T-score < -2.5
- Osteopenia: T-score -0 to -2.5
- Many healthy people, especially above the age of 50, have BMD values in the osteopenic range.
- Normal: BMD -0 to +2.5
- Osteosclerotic diseases and OA: > +5

Results need to be interpreted carefully. It is possible for BMD values to lie in the normal or osteopenic range in patients who have osteoporosis, due to coexisting conditions such as aortic calcification, osteophytes, spinal deformity, vertebral compression fractures, degenerative disc disease and OA. The abnorma appearances should be confirmed by X-ray or other imaging as appropriate.
Advantage :
- It is precise, accurate, uses low doses of radiation and is the ‘gold standard’ in osteoporosis diagnosis